Chapter 16 Skeleton and Movement
1. Choose the correct option
Question (A).
The functional unit of striated muscle is …………..
a. cross-bridges
b. myofibril
c. sarcomere
d. z-band
Answer:
c. sarcomere
Question (B).
A person slips from the staircase and breaks his ankle bone. Which bones are involved?
a. Carpals
b. Tarsal
c. Metacarpals
d. Metatarsals
Answer:
b. Tarsal
Question (C).
Muscle fatigue is due to the accumulation of ……..
a. pyruvic acid
b. lactic acid
c. malic acid
d. succinic acid
Answer:
b. lactic acid
Question (D).
Which one of the following is NOT antagonistic muscle pair?
a. Flexo-extensor
b. Adductor-abductor
c. Levator-depressor
d. Sphinetro-suprinater
Answer:
d. Sphinetro-suprinater
Question (E).
Swelling of sprained foot is reduced by soaking in hot water containing a large amount of common salt,
a. due to osmosis
b. due to plasmolysis
c. due to electrolysis
d. due to photolysis
Answer:
a. due to osmosis
Question (F).
Role of calcium in muscle contraction is ……….
a. to break the cross bridges as a cofactor in the hydrolysis of ATP
b. to bind with troponin, changing its shape so that the actin filament is exposed
c. to transmit the action potential across the neuromuscular junction.
d. to re-establish the polarisation of the plasma membrane following an action potential
Answer:
b. to bind with troponin, changing its shape so that the actin filament is exposed
Question (G).
Hyper-secretion of parathormone can cause which of the following disorders?
a. Gout
b. Rheumatoid arthritis
c. Osteoporosis
d. Gull’s disease
Answer:
c. Osteoporosis
Question (H).
Select correct option between two nasal bones
Answer:
(c)
Question 2.
Answer the following questions
Question (A).
What kind of contraction occurs in your neck muscles while you are reading your class assignment?
Answer:
- Isometric contractions occur in the neck muscles while reading class assignment.
- These contractions are important for supporting objects in a fixed position.
Question (B).
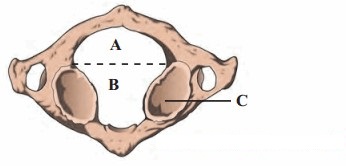
Observe the diagram and enlist importance of ‘A’, ‘B’ and ‘C’.
Answer:
- A – Posterior portion of vertebral foramen of atlas vertebrae; Importance – The spinal cord runs through this portion of vertebral foramen
- B – Anterior portion of vertebral foramen of axis vertebrae; Importance – In this portion, the odontoid process of axis vertebrae forms ‘NO’ joint.
- C – Inferior articular facet; Importance – It articulates with superior articular facet of axis and permits rotatory movement of head.
Question (C).
Raju intends to train biceps; while exercising using dumbbells, which joints should remain stationary and which should move?
Answer:
While performing exercise of biceps using dumbbells, the joint which should remain stationary are wrist joint or radiocarpal joint, ball and socket joint of shoulder. The only joint which should move is hinge joint of elbow.
Question (D).
In a road accident, Moses fractured his leg. One of the passers by, tied a wodden plank to the fractured leg while Moses
was rushed to the hospital Was this essential? Why?
Answer:
- Fracture is a significant and traumatic injury which requires medical attention however, getting timely first aid is important.
- If any bone is fractured, it is essential that the fractured part be immobilized to prevent further injury. It can be done with the help of any available wooden plank or batons or rulers. Thus, a wooden plank was tied to Moses’s fractured leg as a first aid for fracture.
- A fractured bone is immobilized to prevent the sharp edges of the fractured bone from moving and cutting tissue, muscle, blood vessels and nerves. Immobilization can also help reduce pain or control shock.
Question (E).
Sprain is more painful than fracture. Why?
Answer:
- A sprain is an injury that involves the ligaments (tissues that connect bones at joints), whereas a fracture is an injury that involves bones.
- Sprains can be of three degree: 1st degree: Mild with micro-tears, 2nd degree: Partial with visible tear in ligament, 3rd degree: Completely torn ligament.
- If a sprain is 3rd degree, it will be more painful than a fracture. It usually requires a surgery to fix this injury, while breaking a bone, most of the time does not require surgery.
- Breaks or Fractures also vary greatly. Minor fractures (like stress/ hairline fractures) are much less painful than compound/ complex fractures in which the bone may be cracked into half.
- Blood supply is essential for growth and regeneration. Bones are highly vascularized whereas, ligaments are not. This causes the bones to heal comparatively faster than severe sprains. Thus, the duration of enduring pain until the injury heals also differs.
- Also, ligaments have a rich supply of sensory nerves, which may also be responsible for an elevated sense of pain during severe sprains.
[Note: 1st and 2nd degree sprains are not very serious and may be lesser painful than a fracture. Depending on the severity of the injury, intensity of pain will vary.]
Question (F).
Why a red muscle can work for a prolonged period whereas white muscle fibre suffers from fatigue after a shorter work? (Refer to chapter animal tissues.)
Answer:
- Red muscle fibres contain large amount of myoglobin and mitochondria (site of aerobic respiration), whereas white muscles fibres contain lesser amount of myoglobin and mitochondria.
- Myoglobin is an iron-containing pigment that carries oxygen molecules to muscle tissues. Abundance of these pigments in red muscle fibres supports higher rate of aerobic respiration, whereas white muscle fibres have less mitochondria and depend upon anaerobic respiration.
- Anaerobic respiration in muscle white fibres leads to the production of lactic acid and accumulation of higher of levels lactic acid can result in fatigue in white muscle fibres.
Thus, red muscle fibres can perform prolonged work and show less fatigue due to accumulation of negligible amount loss or of lactic acid, whereas white muscle fibres suffer from fatigue after a shorter work due to accumulation of higher amount of lactic acid.
3. Answer the following questions in detail
Question (A).
How is the structure of sarcomere suitable for the contractility of the muscle? Explain its function according to sliding
filament theory. (Refer to chapter animal tissues.)
Answer:
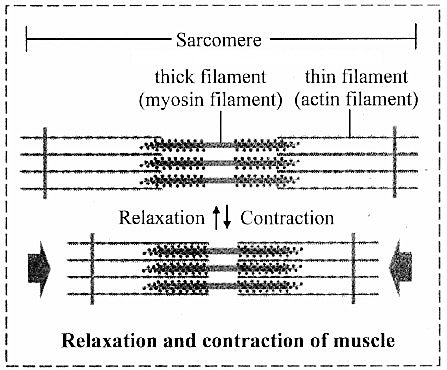
i. Sarcomere is the functional unit of myofibril. It has specific arrangement of actin and myosin filaments. The components of sarcomere are organized into variety of bands and zones. Actin and myosin are referred as contractile proteins. Actin is called as thin filament whereas myosin in called as thick filament. The structure of sarcomere:
ii. ‘A’ band – dark bands present at the centre of sarcomere and contain myosin as well as actin.
‘H’ zone or Hensen’s zone – light area present at the centre of ‘A’ band
‘M’ line – present at the centre of ‘H’ zone
‘I’ band – light bands present on the either side of ‘A’ band containing only actin
Z’ line – adjacent ‘I’ bands are separated by ‘Z’ line.
iii. Sliding filament theory: It was put forth by H.E Huxley and A.F Huxley. It is also known as ‘Walk along theory’ or Ratchet theory.
- According to the sliding filament theory, the interaction between actin and myosin filaments is the basic cause of muscle contraction. The actin filaments are interdigitated with myosin filaments.
- The head of the myosin is joined to the actin backbone by a cross bridge forming a hinge joint. From this joint, myosin head cannot tilt forward or backward. This movement is an active process as it utilizes ATP.
- Myosin head contains ATPase activity. It can derive energy by the breakdown of ATP molecule. This energy can be used for the movement of myosin head.
-
During contraction, the myosin head gets attached to the active site of actin filaments and pull them inwardly so that the actin filaments slide over the myosin filaments. This results in the contraction of muscle fibre.

Question (B).
Ragini, a 50 year old office goer, suffered hair-line cracks in her right and left foot in short intervals of time. She was worried about minor jerks leading to hair line cracks in bones. Doctor explained to her why it must be happening and prescribed medicines.
What must be the cause of Ragini’s problem? Why has it occurred? What precautions she should have taken earlier? What care she should take in future?
Answer:
- Considering Ragini’s age, she may be undergoing menopause. After menopause, oestrogen level declines resulting in lower bone density.
- Osteoporosis:
- In this disorder, bones become porous and hence brittle. It is primarily age related disease and is more common in women than men.
- Osteoporosis may be caused due to decreasing estrogen secretion after menopause, deficiency of vitamin D, low calcium diet, decreased secretion of sex hormones and thyrocalcitonin.
- As age advances, bone resorption outpaces bone formation. Hence, the bones lose mass and become brittle. More calcium is lost in urine, sweat, etc., than it is gained through diet. Thus, prevention of disease is better than treatment by consuming adequate amount of calcium and exercise at young age.
- A person with previous hairline fractures is more susceptible to reoccurrence of fractures. Hence, Ragini needs to take her medications and supplements properly, avoid jerky movements and maintain body weight.
Question (C).
How does structure of actin and myosin help muscle contraction?
Answer:
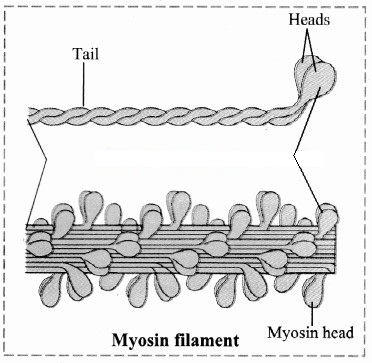
i. Myosin filament:
-
Each myosin filament is a polymerized protein.
Many meromyosins (monomeric proteins) constitute one thick filament. - Myosin molecule consists of two heavy chains (heavy meromyosin / HMM) coiled around each other forming a double helix. One end of each of these chains is projected outwardly is known as cross bridge. This end folds to form a globular protein mass called myosin head.
- Two light chains are associated with each head forming 4 light chains/light meromyosin / LMM.
- Myosin head has a special ATPase activity. It can split ATP to produce energy.
- Myosin contributes 55% of muscle proteins.
-
In sarcomere, myosin tails are arranged to point towards the centre of the sarcomere and the heads point to the sides of the myofilament band.

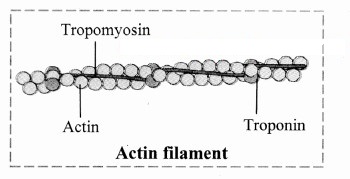
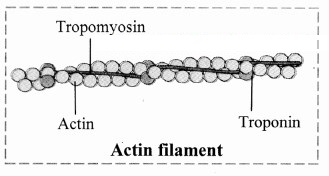
ii. Actin filament: It is a complex type of contractile protein. It is made up of three components:
- F actin: It forms the backbone of actin filament. F actin is made up of two helical strands. Each strand is composed of polymerized G actin molecules. One ADP molecule is attached to G actin molecule.
- Tropomyosin: The actin filament contains two additional protein strands that are polymers of tropomyosin molecules. Each strand is loosely attached to an F actin. In the resting stage, tropomyosin physically covers the active myosin-binding site of the actin strand.
-
Troponin: It is a complex of three globular proteins, is attached approx. 2/3rd distance along each tropomyosin molecule. It has affinity for actin, tropomyosin and calcium ions. The troponin complex is believed to attach the tropomyosin to the actin. The strong affinity of troponin for calcium ions is believed to initiate the contraction process.

Question (D).
Justify the structure of atlas and axis vertebrae with respect to their position and function.
Answer:
i. Atlas vertebrae:
- Atlas is the ring-like, 1st cervical vertebrae. It has anterior, posterior arches and large lateral masses.
- It lacks centrum and spinous process. The superior surfaces of the lateral masses are concave and are known as superior articular facets.
- These facets articulate with the occipital condyles of the occipital bone thereby forming atlanto-occipital joints. This articulation permits ‘YES movement’ or nodding movement.
- The inferior surfaces of the lateral masses known as inferior articular facets articulate with axis vertebrae,
ii. Axis vertebrae:
- It is the 2nd cervical vertebrae.
- A peg-like process called odontoid process projects superiorly through the anterior portion of the vertebral foramen of the atlas.
- The odontoid process forms a pivot on which the atlas and head rotate. This arrangement allows ‘NO movement’ or side to side movement of the head.
- The articulation formed between the anterior arch of atlas, the odontoid process of the axis and between their articular facets is called as atlanto-axial joint.
Question (E).
Observe the blood report given below and diagnose the possible disorder.
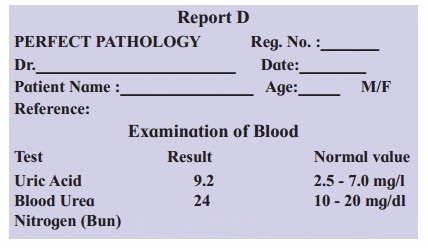
Answer:
On observing Report D, it is clear that the level of uric acid is more than normal, thus the patient must be suffering from gouty arthritis.
Also, the elevated blood urea nitrogen (BUN) indicates dysfunctional liver and/ or kidneys. It generally occurs due to decrease in GFR, caused by renal disease or obstruction of urinary tract.
Question 4.
Write short notes on following points
Question (A).
Actin filament
Answer:
Actin filament: It is a complex type of contractile protein. It is made up of three components:
- F actin: It forms the backbone of actin filament. F actin is made up of two helical strands. Each strand is composed of polymerized G actin molecules. One ADP molecule is attached to G actin molecule.
- Tropomyosin: The actin filament contains two additional protein strands that are polymers of tropomyosin molecules. Each strand is loosely attached to an F actin. In the resting stage, tropomyosin physically covers the active myosin-binding site of the actin strand.
-
Troponin: It is a complex of three globular proteins, is attached approx. 2/3rd distance along each tropomyosin molecule. It has affinity for actin, tropomyosin and calcium ions. The troponin complex is believed to attach the tropomyosin to the actin. The strong affinity of troponin for calcium ions is believed to initiate the contraction process.

Question (B).
Myosin filament
Answer:
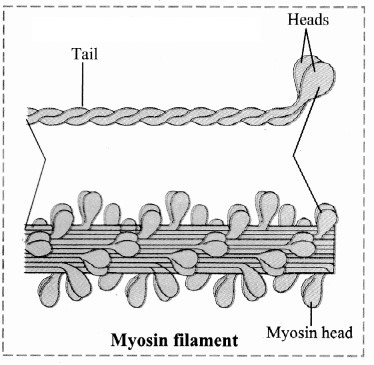
i. Myosin filament:
-
Each myosin filament is a polymerized protein.
Many meromyosins (monomeric proteins) constitute one thick filament. - Myosin molecule consists of two heavy chains (heavy meromyosin / HMM) coiled around each other forming a double helix. One end of each of these chains is projected outwardly is known as cross bridge. This end folds to form a globular protein mass called myosin head.
- Two light chains are associated with each head forming 4 light chains/light meromyosin / LMM.
- Myosin head has a special ATPase activity. It can split ATP to produce energy.
- Myosin contributes 55% of muscle proteins.
-
In sarcomere, myosin tails are arranged to point towards the centre of the sarcomere and the heads point to the sides of the myofilament band.

Question (C).
Role of calcium ions in contraction and relaxation of muscles.
Answer:
Calcium ions play a major role in contraction and relaxation of muscles.
- Calcium ions are released from the sarcoplasm during muscle contraction and stored in sarcoplasmic reticulum during muscle relaxation.
- When a skeletal muscle is excited and an action potential travels along the T tubule, the concentration of calcium ions increases.
- These calcium ions bind to troponin which in turn undergoes a conformational change that causes tropomyosin to move away from the myosin-binding sites on actin. Once these binding sites are free, myosin heads bind to them to form cross-bridges and the muscle fiber contracts.
- The decrease in calcium ion concentration in the sarcoplasmic reticulum causes tropomyosin to slide back and block the myosin binding sites on actin. This causes the muscle to relax.
Question 5.
Draw labelled diagrams
Question (A).
Synovial joint.
Answer:
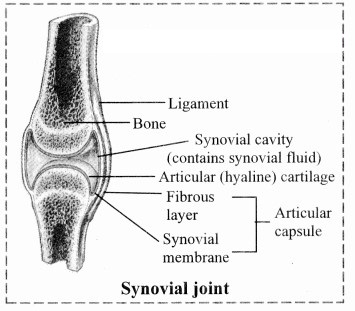
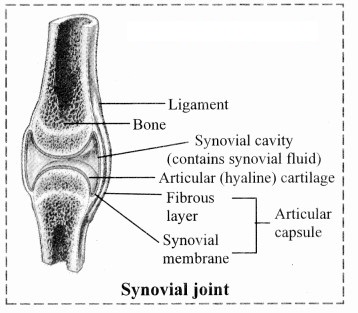
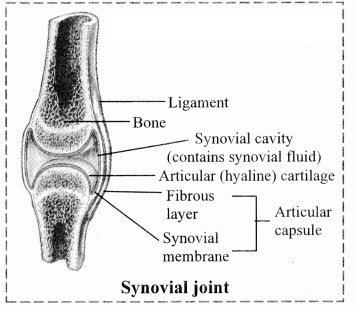
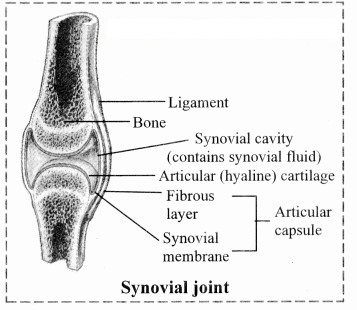
i. Synovial joints / freely movable joints / diarthroses:
- It is characterized by presence of a space called synovial cavity between articulating bones that renders free movement at the joint.
- The articulating surfaces of bones at a synovial joint are covered by a layer of hyaline cartilage. It reduces friction during movement and helps to absorb shock.
-
Synovial cavity is lined by synovial membrane that forms synovial capsule. Synovial membrane secretes synovial fluid.

-
Synovial fluid is a clear, viscous, straw coloured fluid similar to lymph. It is viscous due to hyaluronic acid. The synovial fluid also contains nutrients, mucous and phagocytic cells to remove microbes.
Synovial fluid lubricates the joint, absorbs shocks, nourishes the hyaline cartilage and removes waste materials from hyaline cartilage cells (as cartilage is avascular). Phagocytic cells destroy microbes and cellular debris formed by wear and tear of the joint. - If the joint is immobile for a while, the synovial fluid becomes viscous and as joint movement starts, it becomes less viscous.
- The joint is provided with capsular ligament and numerous accessory ligaments. The fibrous capsule is attached to periosteum of articulating bones. The ligament helps in avoiding dislocation of joint.
- The types of synovial joints are on follows:
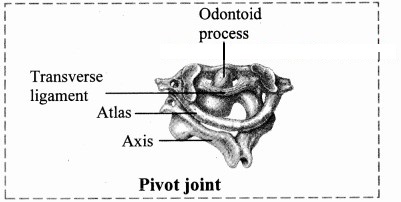
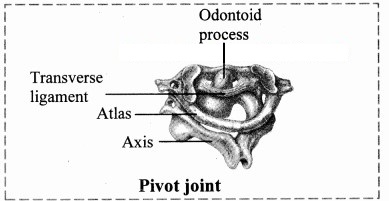
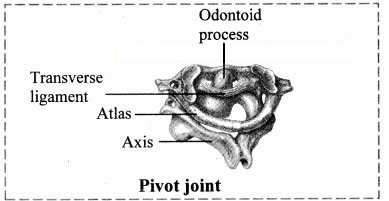
1. Pivot joint: In this type of joint, the rounded or pointed surface of one bone articulates with a ring formed partly by another bone and partly by the ligament. Rotation only around its own longitudinal axis is possible. e.g. in joint between atlas and axis vertebrae, head turns side ways to form ‘NO’ joint.
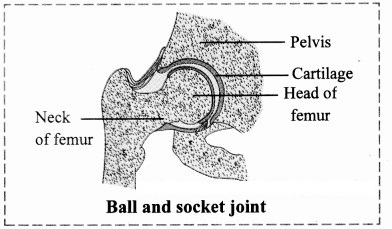
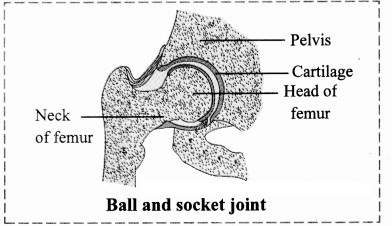
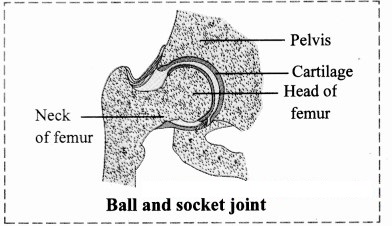
2. Ball and socket joint: The ball like surface of one bone fits into cup like depression of another bone forming a movable joint. Multi-axial movements are possible. This type of joint allows movements along all three axes and in all directions. e.g. Shoulder and hip joint.
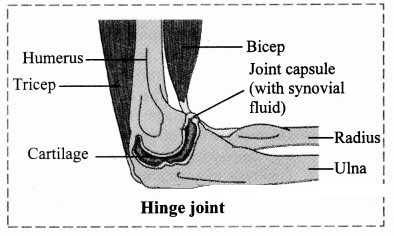
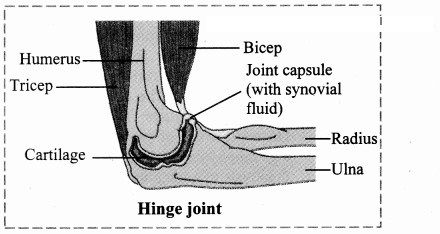
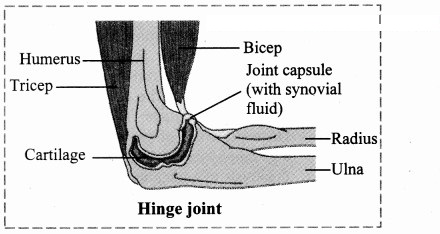
3. Hinge joint: In a hinge joint, convex surface of one bone fits into concave surface of another bone. In most hinge joints one bone remains stationary and other moves. The angular opening and closing motion (like hinge) is possible. In this joint only mono-axial movement takes place like flexion and extension. e.g. Elbow and knee joint.
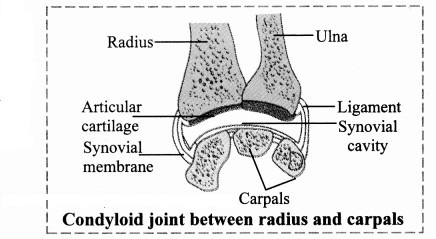
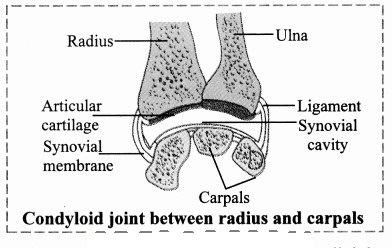
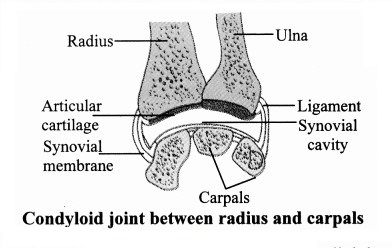
4. Condyloid joint: It is an ellipsoid joint. The convex oval shaped projection of one bone fits into oval shaped depression in another bone. it is a biaxial joint because it permits movement along two axes viz, flexion, extension, abduction, adduction and circumduction is possible. e.g. Metacarpophalangeal joint.
5. Gliding joint: It is a planar joint, where the articulating surfaces of bones are flat or slightly curved. These joints are non-axial because the motion they allow does not occur along an axis or a plane. e.g. Intercarpal and intertarsal joints.
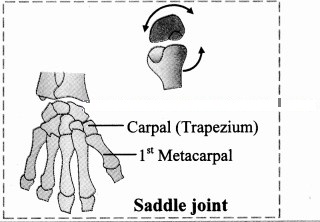
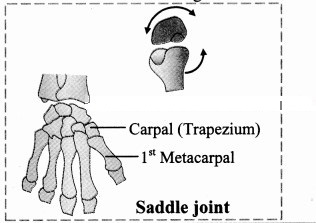
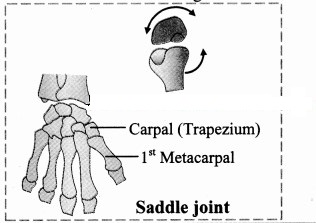
6. Saddle joint: This joint is a characteristic of Homo sapiens. Here the articular surface of one bone is saddle-shaped and that of other bone fits into saddle (each bone forming this joint have both concave and convex areas). It is a modified condyloid joint in which movement is somewhat more free. It is a biaxial joint that allows flexion, extension, abduction, adduction and circumduction.
e.g. Carpometacarpellar joint between carpal (trapezium) and metacarpal of thumb.
Question (B).
Different cartilagenous joints.
Answer:
Cartilaginous / slightly movable joints / amphiarthroses:
These joints are neither fixed nor freely movable. Articulating bones are held together by hyaline or fibrocartilages. They are further classified as
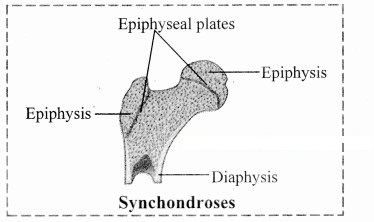
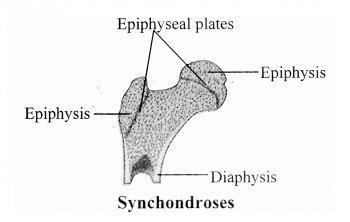
a. Synchondroses: The two bones are held together by hyaline cartilage. They are meant for growth. On completion of growth, the joint gets ossified, e.g. Epiphyseal plate found between epiphysis and diaphysis of a long bone, Rib – Sternum junction.
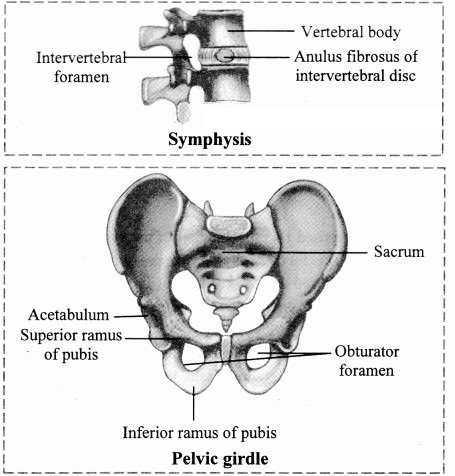
b. Symphysis: In this type of joint, broad flat disc of fibrocartilage connects two bones. It occurs in mid-line of the body. e.g. Intervertebral discs, manubrium and sternum, pubic symphysis.
Practical / Project :
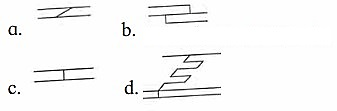
Identify the following diagrams and demonstrate the concepts in classroom.
Answer:
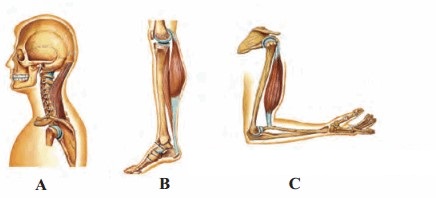
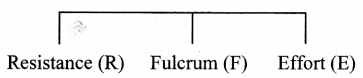
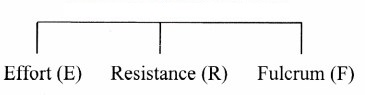
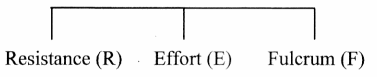
The diagrams A, B and C represent Class I, Class II and Class III lever respectively.
For description:
-
Class I lever: The joint between the first vertebra and occipital condyle of skull is an example of Class I lever. The force is directed towards the joints (fulcrum); contraction of back muscle provides force while the part of head that is raised acts as

-
Class II lever: Human body raised on toes is an example of Class II lever. Toe acts as fulcrum, contracting calf muscles provide the force while raised body acts as resistance.

-
Class III lever: Flexion of forearm at elbow exhibit lever of class III. Elbow joint acts as fulcrum and radius, ulna provides resistance. Contracting bicep muscles provides force for the movement.


[Students are expected to perform the given activity on their own]
Intext Questions and Answers
Movements And Locomotion (Textbook Page No. 193)
Question 1.
Streaming of protoplasm, peristalsis, walking, running, etc. Which of the above-mentioned movements are internal? Which are external? Can you add few more examples?
Answer:
- Streaming of protoplasm, peristalsis are internal movements. Walking and running are external movements.
- Examples of internal movement: Contraction and relaxation heart, inspiration and expiration, contraction of blood vessels, etc.
- Examples of external movement: Swimming; movement tongue, jaws, snout, tentacles, movement of ear pinna, etc.
Can you recall? (Textbook Page No. 193)
Question 1.
Which are different types of muscular tissues?
Answer:
- Smooth / non-striated / visceral / involuntary muscles
- Cardiac muscles
- Skeletal / straited / voluntary muscles.
Question 2.
Name the type of muscles which bring about running and speaking.
Answer:
Skeletal muscles (Voluntary muscles)
Question 3.
Name the muscles which do not contract as per our will.
Answer:
Involuntary muscles (smooth muscles and cardiac muscles)
Question 4.
Which type of muscles show rhythmic contractions?
Answer:
Cardiac muscles
Question 5.
Which type of muscle is present in the diaphragm of the respiratory system?
Answer:
Skeletal muscle
Question 6.
State the functions of:
- Smooth muscles
- Cardiac muscles
- Striated muscles
Answer:
- Smooth muscles: They bring about involuntary movements like peristalsis in the alimentary canal, constriction and dilation of blood vessels.
- Cardiac muscles: They bring about contraction and relaxation of the heart.
- Striated muscles: They control voluntary movements of limbs, head, trunk, eyes, etc.
Can you recall? (Textbook Page No. 193)
Question 1.
Name the part of human skeleton situated along the vertical axis.
Answer:
Axial skeleton
Question 2.
Give an account of bones of human skull.
Answer:
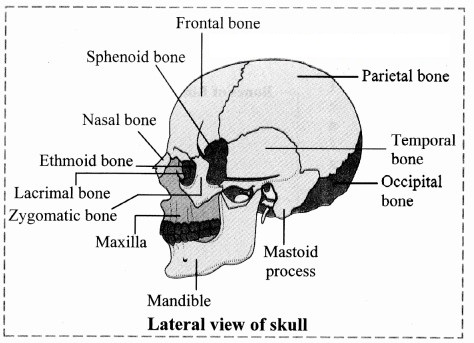
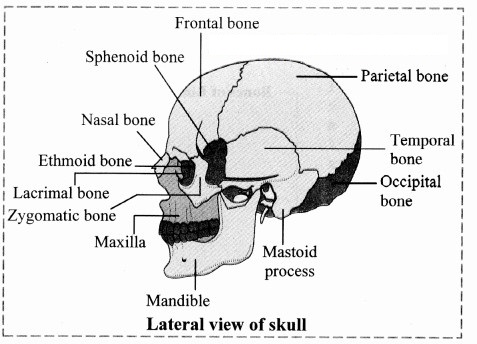
Skull is made up of 22 bones. It is located at the superior end of vertebral column. The bones of skull are
joined by fixed or immovable joints except for jaw.
Skull consists of cranium or brain box and facial bones.
i. Cranium: It is made up of four median bones and two paired bones.
- Frontal bone: It is median bone (unpaired) forming forehead, roof of orbit (eye socket) and the most anterior part of cranium. It is connected to two parietals, sphenoid and ethmoid bone.
- Parietal bones: These paired bones form the roof of cranium and greater portion of sides of the cranium.
- Temporal bones: These paired bones are situated laterally just above the ear on either side. Each temporal bone gives out zygomatic process that joins zygomatic bone to form zygomatic arch. Just at the base of zygomatic process is mandibular fossa, a depression for mandibles (lower jaw bone) that forms the only movable joint of the skull. This bone harbors the ear canal that directs sound waves into the ear. The processes of temporal bones provide points for attachment for various muscles of neck and tongue.
- Occipital bone: It is a single bone present at the back of the head. It forms the posterior part and most of the base of cranium. The inferior part of this bone shows foramen magnum, the opening through which medulla oblongata connects with spinal cord. On the either sides of foramen magnum are two prominent protuberances called occipital condyles. These fit into the corresponding depressions present in 1st vertebra.
- Sphenoid bone: Median bone present at the base of the skull that articulates with all other cranial bones and holds them together. This butterfly shaped bone has a saddle shaped region called sella turcica. In this hypophyseal fossa, the pituitary gland is lodged.
- Ethmoid bone: This median bone is spongy in appearance. It is located anterior to sphenoid and posterior to nasal bones. It contributes to formation of nasal septum and is major supporting structure of nasal cavity.
ii. Facial Bones: Fourteen facial bones give a characteristic shape to the face. The growth of face stops of the
age of 16.
Following bones comprise the facial bones:
- Nasals: These are paired bones that form the bridge of nose.
- Maxillae: These form the upper jaw bones. They are paired bones that join with all facial bones except mandible. Upper row of teeth are lodged maxillae.
-
Palatines: These are paired bones forming the roof of buccal cavity or floor of the nasal cavity.

- Zygomatic bones: They are commonly called as cheek bones.
-
Lacrimal bones: These are the smallest amongst the facial bones.
These bones form the medial wall of each orbit. They have lacrimal fossa that houses lacrimal sacs. These sacs gather tears and send them to nasal cavity. - Inferior nasal conchae: They form the part of lateral wall of nasal cavity. They help to swirl and filter air before it passes to lungs.
- Vomer: The median, roughly triangular bone that forms the inferior portion of nasal septum.
- Mandible: This median bone forms the lower jaw. It is the largest and strongest facial bone. It is the only movable bone of skull. It has curved horizontal body and two perpendicular branches i.e. rami. These help in attachment of muscles. It has lower row of teeth lodged in it.
Think about it. (Textbook Page No. 193)
Question 1.
Did you ever feel tickling in muscles?
Answer:
Yes, the tickling sensation in muscles can be felt and sometimes it is also accompanied by itching sensation.
Question 2.
What is locomotion?
Answer:
The change in locus of whole body of living organism from one place to another place is called locomotion.
Question 3.
State the four basic types of locomotory movements seen in animals.
Answer:
The four basic types locomotory movements seen in animals are:
- Amoeboid movement: It is performed by pseudopodia, e.g. leucocytes.
- Ciliary movement: It is performed by cilia, e.g. ciliated epithelium. In Paramoecium, cilia help in passage of food through cytopharynx.
- Whirling movement: It is performed by flagella, e.g. sperms.
- Muscular movement: It is performed by muscles, with the help of bones and joints.
Question 1.
Why do muscles show spasm after rigorous contraction?
Answer:
- Rigorous contraction of muscles occurs during strenuous activities (swimming. running, cycling, aerobics. etc.)
- Muscle contraction requires energy. Glucose in muscle cells breakdown during anerobic respiration resulting in accumulation of lactic acid.
- This lactic acid buildup triggers muscle spasm around muscle cells.
Question 2.
Why do we shiver during winter?
Answer:
- Humans are homeotherms as the can regulate their body temperature with respect to the surrounding temperature. During winter, when temperature falls, the thermoreceptors detect the change in temperature and send signals to the brain.
- Shivering reflex i.e. rapid contraction of muscles is triggered by the brain to generate heat and raise the body temperature.
Can you tell? (Textbook Page No. 194)
Question 1.
Why are movement and locomotion necessary among animals?
Answer:
-
Movement is one of the important characteristics of all the living organisms. Animals exhibit wide range of
movements like rhythmic beating of heart, movement of diaphragm during respiration, ingestion of food,
movement of eyeballs, etc. - Locomotion results into change in place or location of an organism. Animals locomote in search of food, mate, shelter, breeding ground. while escaping from the enemy, etc.
- Thus, locomotion and movement are necessary to support the living of animals.
Question 2.
All locomotions are movements but all movements are not locomotion. Justify
Answer:
Locomotion occurs when body changes its position, however all movements may not result in locomotion. Thus, all locomotions are movements but all movements are not locomotion.
Question 3.
Kriti was diagnosed with knee tendon injury. She asked the doctor whether she will be able to walk due to the injury? If not then state the reason.
Answer:
Knee tendon injury affects the ability to walk. Kriti may not be able to walk freely as the tendons attached to the bones help in the movement of the parts of skeleton.
Question 4.
What are antagonistic muscles? Explain with example.
Answer:
- The muscles that work in pairs and produce opposite action are known as antagonistic muscles, e.g. biceps and triceps of upper arm.
- The biceps (flexors) bring flexion (folding) and triceps (extensors) bring extension of the elbow joint.
- One member from a pair is capable of bending the joint by pulling of bones the other member is capable of straightening the same joint by pulling.
- In antagonistic pair of muscles, one member is stronger than the other, e.g. The biceps are stronger than the triceps.
Question 5.
Describe the antagonistic muscles in detail.
Answer:
Following are the important antagonistic muscles:
- Flexor and extensor: Flexor muscle on contraction results into bending or flexion of joint, e.g. Biceps. Extensor muscle on contraction results in straightening or extension of a joint, e.g. Triceps.
- Abductor and adductor: Abductor muscle moves a body part away from the body axis. e.g. Deltoid muscle of shoulder moves the arm away from the body. Adductor muscle moves a body part towards the body axis, e.g. Latissimus dorsi of shoulder moves the arm near the body.
- Pronator and supinator: Pronator turns the palm downwards and supinator turns the palm upward.
- Levator and depressor: Levator raises a body part and the depressors lower the body part.
- Protractor and retractor: Protractor moves forward, whereas the retractor moves backward.
- Sphincters: Circular muscles present in the inner walls of anus, stomach, etc., for closure and opening.
Question 6.
Differentiate between:
i. Flexor and extensor muscles
Answer:
Flexor Muscles | Extensor Muscles | ||
a. | Flexor muscles contract and bring about the bending or flexion of joint. | a. | Extensor muscles contract and bring about the straightening or extension of joint. |
b. | These muscles decrease the angle between the bones on two sides of a joint. | b. | These muscles increase the angle between the components of limb. |
e.g. | Biceps | e.g. | Triceps |
ii. Pronator and supinator: Pronator turns the palm downwards and supinator turns the palm upward.
Can you recall? (Textbook Page No. 194)
Question 1.
Comment on contraction of skeletal muscles.
Answer:
Skeletal muscles show quick and strong voluntary contractions. They bring about voluntary movements of the body. For mechanism of muscle contraction:
When the muscles are relaxed, the active sites remain covered with tropomyosin and troponin complex. Due to this, myosin cannot interact with active site of actin and thus contraction cannot occur.
- When an impulse (action potential) comes to muscle through motor end plate, it spreads throughout the sarcolemma of the myofibril.
- The transverse tubules of sarcoplasmic reticulum release large number of Ca++ ions into sarcoplasm. These calcium ions interact with the troponin molecules and the interaction inactivates troponin-tropomyosin complex. This causes change in the structure of tropomyosin.
- As a result, tropomyosin gets detached from the active site of actin (F actin) filament, exposing the active site for actin.
- The myosin head cleaves the ATP to derive energy and gets attached to the uncovered active site of actin. This results into the formation of acto-myosin complex.
- The myosin heads are now tilted backwards and pull the attached actin filament inwardly. This results in contraction of the muscle fibres.
Do You Know How (Textbook Page No. 195)
Question 1.
Do skeletal muscles contract and bring about movement and locomotion?
Answer:
When the muscles are relaxed, the active sites remain covered with tropomyosin and troponin complex. Due to this, myosin cannot interact with active site of actin and thus contraction cannot occur.
- When an impulse (action potential) comes to muscle through motor end plate, it spreads throughout the sarcolemma of the myofibril.
- The transverse tubules of sarcoplasmic reticulum release large number of Ca++ ions into sarcoplasm. These calcium ions interact with the troponin molecules and the interaction inactivates troponin-tropomyosin complex. This causes change in the structure of tropomyosin.
- As a result, tropomyosin gets detached from the active site of actin (F actin) filament, exposing the active site for actin.
- The myosin head cleaves the ATP to derive energy and gets attached to the uncovered active site of actin. This results into the formation of acto-myosin complex.
- The myosin heads are now tilted backwards and pull the attached actin filament inwardly. This results in contraction of the muscle fibres.
Internet my friend. (Textbook Page No. 196)
Question 1.
Collect information about‘T’ tubules of sarcoplasmic reticulum.
Answer:
- T tubules or the transverse tubules are invaginations of the sarcolemma penetrating into the myocyte interior, forming a highly branched and interconnected network that makes junctions with the sarcoplasmic reticulum.
- These tubules are selectively enriched with specific ion channels and proteins crucial in the development of calcium transients necessary in excitation-contraction coupling, thereby facilitating a fast-synchronous contraction of the entire cell volume.
-
They are unique to straited muscle cells.
[Source: https://www. uniprot. org/locations]
Can you tell? (Textbook Page No. 197)
Question 1.
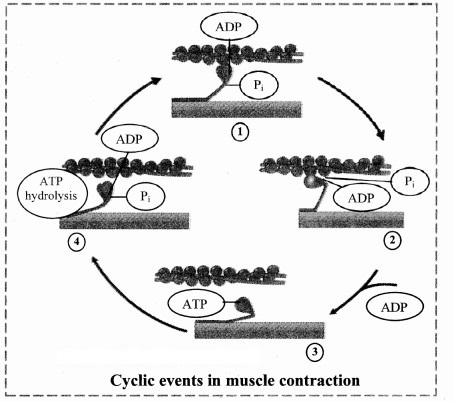
Explain the chemical changes taking place in muscle contraction.
Answer:
The muscle undergoes various chemical changes during contraction, they are as follows:
- A nerve impulse arrives at the motor nerve. The neurotransmitter – acetylcholine is released at the neuromuscular junction (N-M junction or motor endplate) enters into the sarcomere.
- This leads to inflow of Na+ inside the sarcomere and generates an action potential in the muscle fibre.
- The action potential passes down the T tubules and activates calcium channels in the T tubular membrane. Activation of calcium channel allows calcium ions to pass into the sarcoplasm. These Ca++ ions binds to the specific sites on troponin of actin filaments and a conformational change occurs in the troponin – tropomyosin complex, thereby removing the masking of active sites for myosin on the actin filament.
- In the myosin head, the enzyme ATPase gets activated in the presence of Ca++ and converts ATP into ADP and inorganic phosphate.
- This energy from ATP hydrolysis is utilized by myosin bridges or myosin heads to bind with active sites of actin and form actomyosin complex pulling the actin filaments towards the centre of sarcomere. The myosin heads are now tilted backwards and pull the attached actin filament inwardly towards them. The actin filament slides over mysosin and contraction occurs.
- Also, the ADP needs to be converted back to ATP immediately as they required for muscular contraction, This is achieved in the muscles by the presence of another high energy compound, creatine phosphate.
- ADP combines with creatine phosphate to produce ATP and creatinine due to which the supply of ATP for muscle contraction is restored but the level of creatine phosphate keeps decreasing and the level of creatinine keeps on increasing.
- The creatinine formed needs to be reconverted to creatine phosphate. This is done by ATP produced during oxidation of glycogen through glycolysis.
Question 2.
Why are muscle rich in creatine phosphate?
Answer:
- Creatine phosphate or phosphocreatine is formed from ATP, when the muscle is in relaxed state. It is a phosphorylated form of creatine.
- Muscle cells contain creatine phosphate which acts as energy reserve as this high energy compound acts as a phosphate donor for ATP formation.
- ATP acts as an immediate source of energy for contraction
Question 3.
Explain the mechanism of muscle contraction and relaxation.
Answer:
Mechanism of muscle contraction:
When the muscles are relaxed, the active sites remain covered with tropomyosin and troponin complex. Due to this, myosin cannot interact with active site of actin and thus contraction cannot occur.
- When an impulse (action potential) comes to muscle through motor end plate, it spreads throughout the sarcolemma of the myofibril.
- The transverse tubules of sarcoplasmic reticulum release large number of Ca++ ions into sarcoplasm. These calcium ions interact with the troponin molecules and the interaction inactivates troponin-tropomyosin complex. This causes change in the structure of tropomyosin.
- As a result, tropomyosin gets detached from the active site of actin (F actin) filament, exposing the active site for actin.
- The myosin head cleaves the ATP to derive energy and gets attached to the uncovered active site of actin. This results into the formation of actomyosin complex.
- The myosin heads are now tilted backwards and pull the attached actin filament inwardly. This results in contraction of the muscle fibres.
Muscle relaxation: During relaxation, all the events occur in reverse direction as that of muscle contraction.
- When the stimulation is terminated, the actomyosin complex is broken down and myosin head gets detached from actin filaments. This process utilizes ATP.
-
Also, the Ca++ ions are pumped back into the sarcoplasmic reticulum. This process too is an energy dependent process and utilizes ATP.

- As a result, the troponin-tropomyosin complex is restored again which covers the active sites of act in filament, due to disappearance of the Ca++ ions. The interaction between actin and myosin ceases and the actin filaments return back to their original position.
- This results in muscle relaxation.
Question 4.
What do you understand by muscle twitch?
Answer:
Single muscle twitch:
Single muscle twitch: It is a muscle contraction initiated by a single brief-stimulation. It occurs in 3 stages: a latent period of no contraction, a contraction period and a relaxation period.
- The involuntary contraction of muscle fibers is known as muscle twitch.
- Muscle twitch is also known as fasciculation.
- It is caused due accumulation of lactic acid in muscles.
Do You Know How (Textbook Page No. 198)
Question 1.
Exoskeletal components change from lower to higher group of animals. These include chitinous structures, nails, horns, hooves, scales, hair, shell, plates, fur, muscular foot, tube feet, etc.
Question 1.
Do you know any of these exoskeletal structures help in movement and locomotion?
Answer:
Nails, hooves, scales, plates, muscular foot and tube feet help in movement and locomotion.
Question 2.
How do scales and plates help in movement and locomotion?
Answer:
Scales and plates in reptiles like snakes provide grip to move on rough edgy surfaces.
Question 3.
Are scales of a fish and that of snake similar?
Answer:
Fishes have dermal scales (bony scales), whereas reptiles like snakes have epidermal scales or scutes (horny, tough extensions of outer layer of skin i.e., stratum corneum).
Question 4.
Find out more information about exoskeletal structures and their role in movement and locomotion.
Answer:
Exoskeletal structures: Exoskeleton provide support, help in movement and also provides protection from predators. The exoskeletal structures vary from organism to organism. Echinoderms have tube feet for locomotion whereas molluscs (e.g. Chiton) have muscular foot for movement and locomotion
[Students are expected to find out more information about exoskeletal structures on their own.]
Question 2.
Name the tissues that form the structural framework of the body.
Answer:
Cartilage and bone
Do you remember? (Textbook Page No. 198)
Question 1.
What are the components of skeletal system?
Answer:
The components of skeletal system are bones, tendons, ligaments and joint.
Question 2.
What type of bones are present in our body?
Answer:
Long bones, short bones, flat bones, irregular bones and sesamoid bones.
Question 3.
How do bones help in various ways?
Answer:
- Bones form the framework of our body and thus provide shape to the body.
- They protect vital organs thus help in the smooth functioning of body.
- The joints between the bones help in movement and locomotion.
- They provide firm surface for attachment of muscles.
- They are reservoirs of calcium and form important site for hemopoiesis.
Use your brain power. (Textbook Page No. 198)
Question 1.
Can you compare bone, muscle and joint which help in locomotion with any simple machines you have studied earlier?
Answer:
Bone, muscle and joint can be compared to the simple machines called levers. Joints act as fulcrum, respective muscle generates the force required to move the bone associated with joint.
Question 2.
Explain the three types of lever found in human body.
Answer:
The three types of lever are as follows:
-
Class I lever: The joint between the first vertebra and occipital condyle of skull is an example of Class I lever. The force is directed towards the joints (fulcrum); contraction of back muscle provides force while the part of head that is raised acts as resistance.

-
Class II lever: Human body raised on toes is an example of Class II lever. Toe acts as fulcrum, contracting calf muscles provide the force while raised body acts as resistance.

-
Class III lever: Flexion of forearm at elbow exhibit lever of class III. Elbow joint acts as fulcrum and radius, ulna provides resistance. Contracting bicep muscles provides force for the movement.

Use your brain power. (Textbook Page No. 199)
Question 1.
Why are long bones slightly bent and not straight?
Answer:
- Long bones include tibia, fibula, femur, humerus, radius, ulna, etc.
- They have greater length than width. They consist of a shaft and variable number of epiphysis.
- They are slightly bent or curved to absorb the stress of the body’s weight and evenly distribute the body weight at several different points.
- If long bones were straight, the weight of the body would be unevenly distributed and the bone would fracture more easily.
Identify and label. (Textbook Page No. 199)
Question 1.
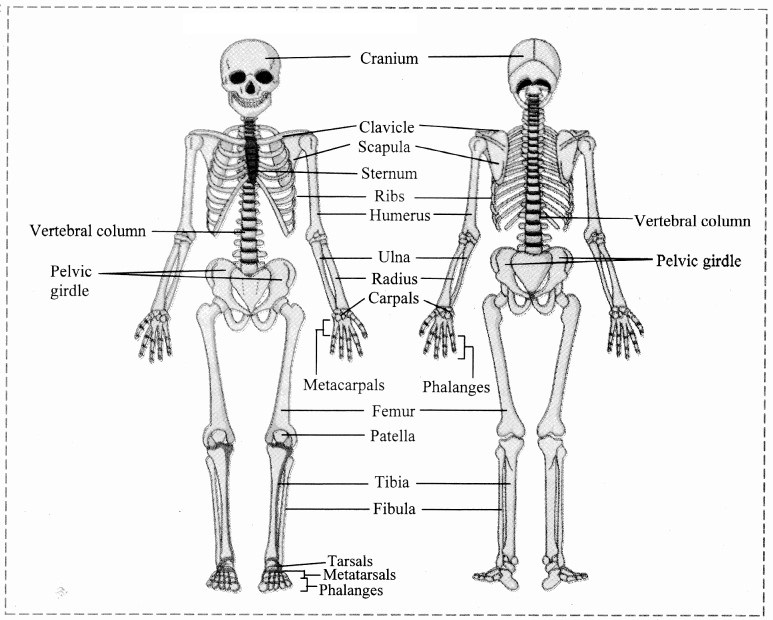
Identify the different bones.
Answer:
Identify and label. (Textbook Page No. 200)
Question 1.
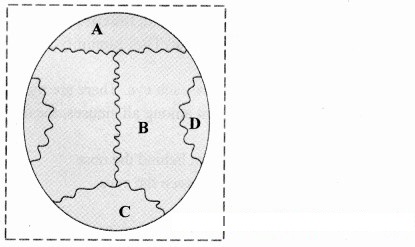
Name A, B, C and D from the given figure and discuss in group.
Answer:
A – Coronal suture,
B – Sagittal suture,
C – Lambdoidal suture,
D – Lateral / Squamous suture
Skull has many sutures (type of immovable joints) present, out of which four prominent ones are:
- Coronal suture: Joins frontal bone with parietals.
- Sagittal suture: Joins two parietal bones.
- Lambdiodal suture: Joins two parietal bones with occipital bone.
- Lateral/squamous sutures: Joins parietal and temporal bones on lateral side.
Can you tell? (Textbook Page No. 201)
Question 1.
Give schematic plan of human skeleton.
Answer:
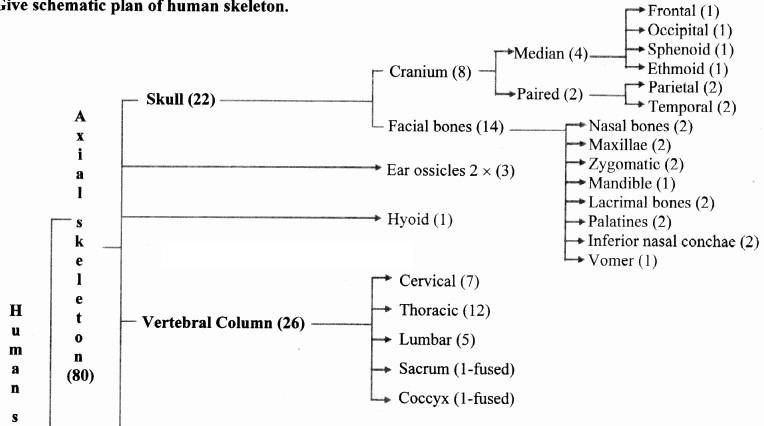
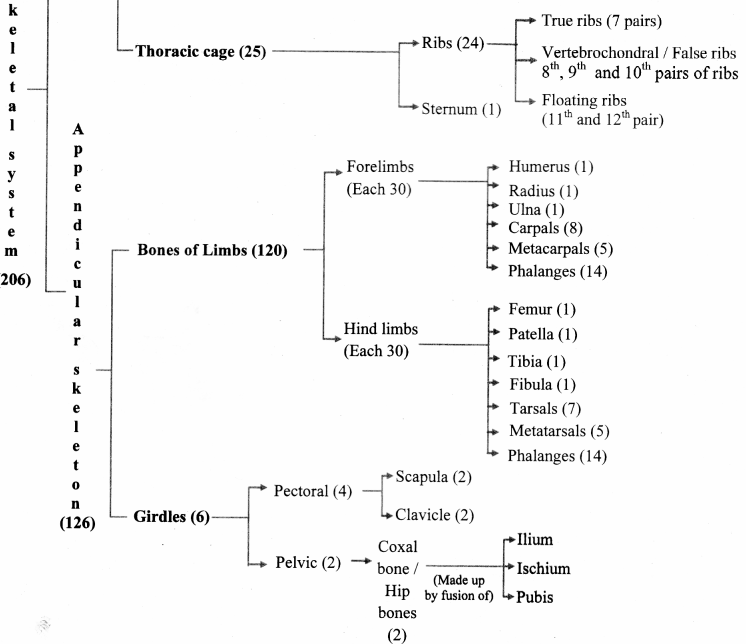
[Note: Numbers in the bracket indicate the number of bones.]
Can you tell? (Textbook Page No. 201)
Question 1.
Enlist the bones of cranium.
Answer:
Cranium: It is made up of four median bones and two paired bones.
- Frontal bone: It is median bone (unpaired) forming forehead, roof of orbit (eye socket) and the most anterior part of cranium. It is connected to two parietals, sphenoid and ethmoid bone.
- Parietal bones: These paired bones form the roof of cranium and greater portion of sides of the cranium.
- Temporal bones: These paired bones are situated laterally just above the ear on either side. Each temporal bone gives out zygomatic process that joins zygomatic bone to form zygomatic arch. Just at the base of zygomatic process is mandibular fossa, a depression for mandibles (lower jaw bone) that forms the only movable joint of the skull. This bone harbors the ear canal that directs sound waves into the ear. The processes of temporal bones provide points for attachment for various muscles of neck and tongue.
- Occipital bone: It is a single bone present at the back of the head. It forms the posterior part and most of the base of cranium. The inferior part of this bone shows foramen magnum, the opening through which medulla oblongata connects with spinal cord. On the either sides of foramen magnum are two prominent protuberances called occipital condyles. These fit into the corresponding depressions present in 1st vertebra.
- Sphenoid bone: Median bone present at the base of the skull that articulates with all other cranial bones and holds them together. This butterfly shaped bone has a saddle shaped region called sella turcica. In this hypophyseal fossa, the pituitary gland is lodged.
- Ethmoid bone: This median bone is spongy in appearance. It is located anterior to sphenoid and posterior to nasal bones. It contributes to formation of nasal septum and is major supporting structure of nasal cavity.
Can you tell? (Textbook Page No. 201)
Question 1.
Write a note on structure and function of skull.
Answer:
i. Structure of skull:
Skull is made up of 22 bones. It is located at the superior end of vertebral column. The bones of skull are joined by fixed or immovable joints except for jaw.
Skull consists of cranium or brain box and facial bones.
i. Cranium: It is made up of four median bones and two paired bones.
- Frontal bone: It is median bone (unpaired) forming forehead, roof of orbit (eye socket) and the most anterior part of cranium. It is connected to two parietals, sphenoid and ethmoid bone.
- Parietal bones: These paired bones form the roof of cranium and greater portion of sides of the cranium.
- Temporal bones: These paired bones are situated laterally just above the ear on either side. Each temporal bone gives out zygomatic process that joins zygomatic bone to form zygomatic arch. Just at the base of zygomatic process is mandibular fossa, a depression for mandibles (lower jaw bone) that forms the only movable joint of the skull. This bone harbors the ear canal that directs sound waves into the ear. The processes of temporal bones provide points for attachment for various muscles of neck and tongue.
- Occipital bone: It is a single bone present at the back of the head. It forms the posterior part and most of the base of cranium. The inferior part of this bone shows foramen magnum, the opening through which medulla oblongata connects with spinal cord. On the either sides of foramen magnum are two prominent protuberances called occipital condyles. These fit into the corresponding depressions present in 1st vertebra.
- Sphenoid bone: Median bone present at the base of the skull that articulates with all other cranial bones and holds them together. This butterfly shaped bone has a saddle shaped region called sella turcica. In this hypophyseal fossa, the pituitary gland is lodged.
- Ethmoid bone: This median bone is spongy in appearance. It is located anterior to sphenoid and posterior to nasal bones. It contributes to formation of nasal septum and is major supporting structure of nasal cavity.
ii. Facial Bones: Fourteen facial bones give a characteristic shape to the face. The growth of face stops of the age of 16.
Following bones comprise the facial bones:
- Nasals: These are paired bones that form the bridge of nose.
-
Maxillae: These form the upper jaw bones. They are paired bones that join with all facial bones except mandible. Upper row of teeth are lodged maxillae.

- Palatines: These are paired bones forming the roof of buccal cavity or floor of the nasal cavity.
- Zygomatic bones: They are commonly called as cheek bones.
- Lacrimal bones: These are the smallest amongst the facial bones. These bones form the medial wall of each orbit. They have lacrimal fossa that houses lacrimal sacs. These sacs gather tears and send them to nasal cavity.
- Inferior nasal conchae: They form the part of lateral wall of nasal cavity. They help to swirl and filter air before it passes to lungs.
- Vomer: The median, roughly triangular bone that forms the inferior portion of nasal septum.
- Mandible: This median bone forms the lower jaw. It is the largest and strongest facial bone. It is the only movable bone of skull. It has curved horizontal body and two perpendicular branches i.e. rami. These help in attachment of muscles. It has lower row of teeth lodged in it.
ii. Functions of skull:
- It protects the brain.
- It provides sockets for ear, nasal chamber and eyes.
- Mandible bone of the skull helps in opening and closing of the mouth.
Internet my friend. (Textbook Page No. 201)
Question 1.
Cleft palate and cleft lip
Answer:
- Cleft palate and cleft lip are the birth defects that occur when a baby’s lip or mouth does develop properly.
- Cleft palate happens when the tissue that forms the roof of the mouth does not join together completely during pregnancy.
- Cleft lip happens when the tissue that makes up the lip does not join completely before birth. This leads to formation of an opening in the upper lip.
[Students are expected to find more information about Cleft Palate and lip on internet.]
Can you tell? (Textbook Page No. 202)
Question 1.
Why skull is important for us? Enlist few reasons.
Answer:
Functions of skull:
- It protects the brain.
- It provides sockets for ear, nasal chamber and eyes.
- Mandible bone of the skull helps in opening and closing of the mouth.
Internet my friend. (Textbook Page No. 202)
Question 1.
Find out information about sinuses present in skull, functions of skull and disorder ‘sinusitis’.
Answer:
Sinuses are the hollow cavities present in the skull. They humidify the air we breathe.
i. The four types of sinuses present in the skull:
- Frontal sinuses: They are located above each eye. There are right and left frontal sinuses.
- Maxillary sinuses: They are the largest among all sinuses, located just behind the cheekbones near to upper jaws.
- Sphenoid sinuses: These are present just behind the nose.
- Ethmoid sinuses: These are present between the eyes.
ii. Functions of skull:
Functions of skull:
- It protects the brain.
- It provides sockets for ear, nasal chamber and eyes.
- Mandible bone of the skull helps in opening and closing of the mouth.
iii. Sinusitis: It is the inflammation of tissue lining the sinuses. Healthy sinuses when get blocked with mucus and germs causing infection which may lead to sinusitis.
[Students are expected to find more information about sinusitis, using the internet.]
Something interesting. (Textbook Page No. 202)
Question 1.
If police suspect strangulation, they carefully inspect hyoid bone and cartilage of larynx. These get fractured during strangulation. V arious such investigations are done in case of suspicious death of an individual where ossification of sutures in skull, width of pelvic girdle, etc. are examined to find out approximate age of victim or gender of victim, etc. You may find out information about forensic science.
Answer:
Forensic science is an application of science which is used in the matter of criminal determination and civil law. It is generally used in investigation of crimes. Forensic scientists collect, preserve and analyze the evidence during the course of investigation.
[Students are expected to find more information about forensic science on internet.]
Try this. (Textbook Page No. 202)
Question 1.
Feel your spine (vertebral column). Is it straight or curved?
Answer:
Our spinc shows four slight curves which are visible when viewed from the sides.
Question 2.
Find information about slipped disc. (Textbook page no.202)
Answer:
- The bones of vertebral column are supported by the intervertebral discs.
- These intervertebral discs act as shock absorbers due to which they are constantly compressed.
- The disc consists of two parts – soft gelatinous inner part (nucleus pulposus) and tough outer ring.
If the ligaments of the intervertebral discs become injured, the pressure developed in the nucleus pulposus protrudes posteriorly or into one of the adjacent vertebrae. This is known as slipped disc.
[Students are expected to find more information using the internet.]
Can you tell? (Textbook Page No. 204)
Question 1.
Write a note on curvatures of vertebral column and mention their importance.
Answer:
- The four curvatures in human spine are cervical, lumbar, thoracic and sacral curvatures.
-
The cervical and lumbar curvatures are secondary and convex whereas the thoracic and sacral curvatures are
primary and concave. -
Importance: Curvatures help in maintaining balance in upright position. They absorb shocks while walking
and also protect the vertebrae from fracture.
Question 2.
Explain the structure of typical vertebra.
Answer:
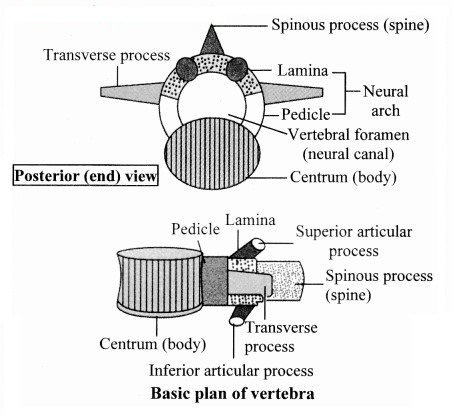
- Each vertebra has prominent central body called centrum.
- The centra of human vertebrae are flat in anterio-posterior aspect. Thus, human vertebrae are amphiplatyan.
- From the either side of the centrum are two thick short processes which unite to form an arch like structure called neural arch, posterior to centrum.
- Neural arch forms vertebral foramen which surrounds the spinal cord.
- Vertebral foramina of all vertebrae form a continuous ‘neural canal’. Spinal cord along with blood vessels and protective fatty covering passes through neural canal.
-
The point where two processes of centrum meet, the neural arch is drawn into a spinous process called neural spine.

- From the base of neural arch, two articulating processes called zygapophyses are given out on either side. The anterior is called superior zygapophyses and posterior called inferior zygapophyses.
- In a stack of vertebrae, inferior zygapophyses of one vertebra articulates with superior zygapophyses of next vertebra. This allows slight movement of vertebrae without allowing them to fall.
- At the junction of zygapophyses, a small opening is formed on either side of vertebra called intervertebral foramen that allows passage of spinal nerve.
- From the base of neural arch, lateral processes are given out called transverse processes. Neural arch, neural spine and transverse processes are meant for attachment of muscles.
Question 2.
How will you identify a thoracic vertebra?
Answer:
Thoracic vertebrae can be identified on the basis of centrum, as the centrum of the thoracic vertebrae is heart shaped.
Can you recall? (Textbook Page No. 206)
Question 1.
How does humerus form ball and socket joint? Where is it located?
Answer:
The head of humerus fits into the glenoid cavity of scapula and forms ball and socket joint. it is located in shoulder and hips.
Can you tell? (Textbook Page No. 208)
Question 1.
Differentiate between the skeleton of palm and foot.
Answer:
Skeleton of palm | Skeleton of foot | |
a. | It consists of metacarpals and phalanges | It consists of metatarsals and phalanges |
b. | Saddle joints and condyloid joints are in the palm. | Condyloid or saddle joints are not present the foot. |
Question 2.
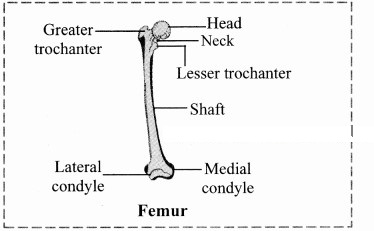
Explain the longest bone in human body.
Answer:
Femur: The thigh bone is the longest bone in the body. The head is joined to shaft at an angle by a short neck. It forms ball and socket joint with acetabulum cavity of coxal bone. The lower one third region of shaft is triangular flattened area called popliteal surface. Distal end has two condyles that articulate with tibia and fibula.
Internet my friend. (Textbook Page No. 212)
Question 1.
Find out information about types of fractures and how they heal.
Answer:
- Fractures are classified based on their severity, shape or position of the fracture line or the physician who first described them.
- Types of fractures:
- Open fractures: The broken ends of the bone protrude through skin.
- Comminuted fractures: The bone is splintered, crushed or broken into pieces at the site of impact and smaller bone fragments lie between the two main fragments.
- Greenstick fractures: A partial fracture in which one side of the bone is broken and the other side bends.
- Impacted fractures: One end of the fractured bone is forcefully driven into the inferior of the other.
- Pott fractures: Fracture of the distal end lateral leg bone with serious injury of the distal tibial articulation.
- Codes fractures: Fracture of the distal end of the lateral forearm in which the distal fragment is displaced posteriorly.
- A fractured bone heals in four phases viz, reactive phase, fibrocartilaginous formation phase, bony callus formation phase and bone remodeling phase.
[Source: Tortora, G., Derrickson, B. Principles of Anatomy and Physiology. 15th Edition]
[Students are expected to find out more information about healing of fractures using the internet.]
Do you remember? (Textbook Page No. 208)
Question 1.
What are joints? What are the types?
Answer:
i. A point where two or more bones get articulated is called joint or articulation or athrosis.
They are classified based on degree of flexibility or movement they permit into lastly synovial or freely movable or diarthroses type of joints.
ii. Synarthroses / fibrous joints / movable joints:
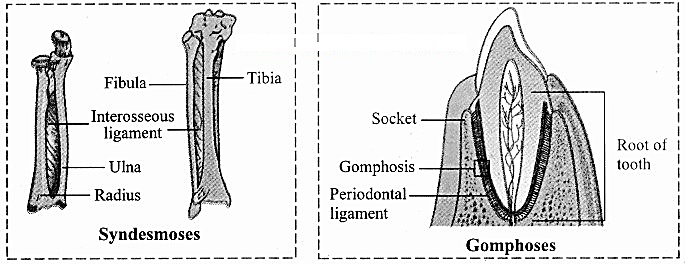
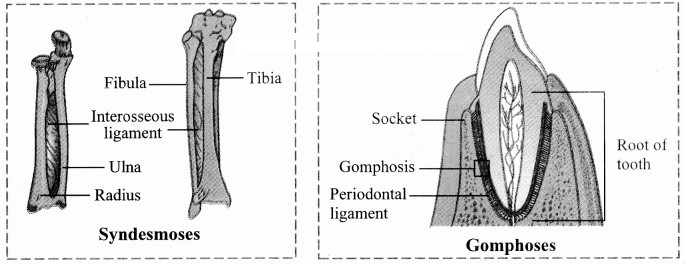
In this joint, the articulating bones are held together by means of fibrous connective tissue. Bones do not exhibit movement. Hence, it is immovable or fixed type of joint. Synarthroses are further classified into sutures, syndesmoses and gomphoses.
- Sutures: It is composed of thin layer of a dense fibrous connective tissue. Sutures are places of growth. They remain open till growth is complete. On completion of growth, they tend to ossify. Sutures may permit some moulding during childhood. Sutures are further classified into butt joint, scarf joint, lap joint and serrate joint.
- Syndesmoses: It is present where there is greater distance between articulating bones. At such locations, fibrous connective tissue is arranged as a sheet or bundle, e.g. Distal tibiofibular joint, interosseous membrane between tibia and fibula and that between radius and ulna.
-
Gomphoses: In this type of joint, a cone shaped bone fits into a socket provided by other bone,
e. g. Tooth and jaw bones.

iii. Cartilaginous / slightly movable joints / amphiarthroses:
These joints are neither fixed nor freely movable. Articulating bones are held together by hyaline or
fibrocartilages. They are further classified as
-
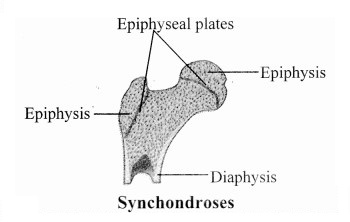
Synchondroses: The two bones are held together by hyaline cartilage. They are meant for growth.
On completion of growth, the joint gets ossified, e.g. Epiphyseal plate found between epiphysis and diaphysis of a long bone, Rib – Sternum junction. -
Symphysis: In this type of joint, broad flat disc of fibrocartilage connects two bones. It occurs in mid-line of the body. e.g. Intervertebral discs, manubrium and sternum, pubic symphysis.

iv. Synovial joints / freely movable joints / diarthroses:
- It is characterized by presence of a space called synovial cavity between articulating bones that renders free movement at the joint.
-
The articulating surfaces of bones at a synovial joint are covered by a layer of hyaline cartilage. It reduces friction during movement and helps to absorb shock.

- Synovial cavity is lined by synovial membrane that forms synovial capsule. Synovial membrane secretes synovial fluid.
- Synovial fluid is a clear, viscous, straw coloured fluid similar to lymph. It is viscous due to hyaluronic acid. The synovial fluid also contains nutrients, mucous and phagocytic cells to remove microbes. Synovial fluid lubricates the joint, absorbs shocks, nourishes the hyaline cartilage and removes waste materials from hyaline cartilage cells (as cartilage is avascular). Phagocytic cells destroy microbes and cellular debris formed by wear and tear of the joint.
- If the joint is immobile for a while, the synovial fluid becomes viscous and as joint movement starts, it becomes less viscous.
- The joint is provided with capsular ligament and numerous accessory ligaments. The fibrous capsule is attached to periosteum of articulating bones. The ligament helps in avoiding dislocation of joint.
g. The types of synovial joints are on follows:
1. Pivot joint: In this type of joint, the rounded or pointed surface of one bone articulates with a ring formed partly by another bone and partly by the ligament. Rotation only around its own longitudinal axis is possible. e.g. in joint between atlas and axis vertebrae, head turns side ways to form ‘NO’ joint.
2. BaIl and socket joint: The ball like surface of one bone fits into cup like depression of another bone forming a movable joint. Multi-axial movements are possible. This type of joint allows movements along all three axes and in all directions. e.g. Shoulder and hip joint.
3. Hinge joint: In a hinge joint, convex surface of one bone fits into concave surface of another bone. In most hinge joints one bone remains stationary and other moves. The angular opening and closing motion (like hinge) is possible. In this joint only mono-axial movement takes place like flexion and extension. e.g. Elbow and knee joint.
4. Condyloid joint: It is an ellipsoid joint. The convex oval shaped projection of one bone fits into oval shaped depression in another bone. It is a biaxial joint because it permits movement along two axes viz, flexion, extension, abduction, adduction and circumduction is possible. e.g. Metacarpophalangeal joint.
5. Gliding joint: It is a planar joint, where the articulating surfaces of bones are flat or slightly curved. These joints are non-axial because the motion they allow does not occur along an axis or a plane. e.g. Intercarpal and intertarsal joints.
Saddle joint: This joint is a characteristic of Homo sapiens. Here the articular surface of one bone is saddle-shaped and that of other bone fits into saddle (each bone forming this joint have both concave and convex areas). It is a modified condyloid joint in which movement is somewhat more free. It is a biaxial joint that allows flexion, extension, abduction, adduction and circumduction. e.g. Carpometacarpellar joint between carpal (trapezium) and metacarpal of thumb.
Imagine. (Textbook Page No. 208)
Question 1.
If your elbow joint would be a fixed type of joint and joint between teeth and gum would be freely movable.
Answer:
- If the elbow joint would be fixed the flexion and extension of the forearm won’t be possible. Also, rotation of the forearm and wrist would not be not possible.
- Gomphoses is the type of joint that holds the teeth in the jaw bone. If this joint would be freely movable, we would not be able to chew and all our teeth would fall out.
Use your brain power. (Textbook Page No. 210)
Question 1.
Why are warming up rounds essential before regular exercise?
Answer:
- Warming up before exercise stimulates the production and secretion of synovial fluid which reduces the stress on joints during exercise.
- Also, if a joint is immobile for a while, the synovial fluid becomes viscous and as joint movement starts, it becomes less viscous.
- Warming up increases the blood circulation, loosening the joints and increasing the blood flow. It also prepares the muscles for physical activity and prevents injuries.
Can you tell? (Textbook Page No. 211)
Question 1.
Classify various types of joints found in human body. Present the information in the form of chart. Give example of each type.
Answer:
i. A point where two or more bones get articulated is called joint or articulation or athrosis.
They are classified based on degree of flexibility or movement they permit into lastly synovial or freely movable or diarthroses type of joints.
ii. Synarthroses / fibrous joints / movable joints:
In this joint, the articulating bones are held together by means of fibrous connective tissue. Bones do not exhibit movement. Hence, it is immovable or fixed type of joint. Synarthroses are further classified into sutures, syndesmoses and gomphoses.
- Sutures: It is composed of thin layer of a dense fibrous connective tissue. Sutures are places of growth. They remain open till growth is complete. On completion of growth, they tend to ossify. Sutures may permit some moulding during childhood. Sutures are further classified into butt joint, scarf joint, lap joint and serrate joint.
- Syndesmoses: It is present where there is greater distance between articulating bones. At such locations, fibrous connective tissue is arranged as a sheet or bundle, e.g. Distal tibiofibular joint, interosseous membrane between tibia and fibula and that between radius and ulna.
-
Gomphoses: In this type of joint, a cone shaped bone fits into a socket provided by other bone,
e. g. Tooth and jaw bones.
iii. Cartilaginous / slightly movable joints / amphiarthroses:
These joints are neither fixed nor freely movable. Articulating bones are held together by hyaline or
fibrocartilages. They are further classified as
-
Synchondroses: The two bones are held together by hyaline cartilage. They are meant for growth.
On completion of growth, the joint gets ossified, e.g. Epiphyseal plate found between epiphysis and diaphysis of a long bone, Rib – Sternum junction. -
Symphysis: In this type of joint, broad flat disc of fibrocartilage connects two bones. It occurs in mid-line of the body. e.g. Intervertebral discs, manubrium and sternum, pubic symphysis.
iv. Synovial joints / freely movable joints / diarthroses:
- It is characterized by presence of a space called synovial cavity between articulating bones that renders free movement at the joint.
-
The articulating surfaces of bones at a synovial joint are covered by a layer of hyaline cartilage. It reduces friction during movement and helps to absorb shock.
- Synovial cavity is lined by synovial membrane that forms synovial capsule. Synovial membrane secretes synovial fluid.
-
Synovial fluid is a clear, viscous, straw coloured fluid similar to lymph. It is viscous due to hyaluronic acid. The synovial fluid also contains nutrients, mucous and phagocytic cells to remove microbes.
Synovial fluid lubricates the joint, absorbs shocks, nourishes the hyaline cartilage and removes waste materials from hyaline cartilage cells (as cartilage is avascular). Phagocytic cells destroy microbes and cellular debris formed by wear and tear of the joint. - If the joint is immobile for a while, the synovial fluid becomes viscous and as joint movement starts, it becomes less viscous.
- The joint is provided with capsular ligament and numerous accessory ligaments. The fibrous capsule is attached to periosteum of articulating bones. The ligament helps in avoiding dislocation of joint.
g. The types of synovial joints are on follows:
1. Pivot joint: In this type of joint, the rounded or pointed surface of one bone articulates with a ring formed partly by another bone and partly by the ligament. Rotation only around its own longitudinal axis is possible. e.g. in joint between atlas and axis vertebrae, head turns side ways to form ‘NO’ joint.
2. BaIl and socket joint: The ball like surface of one bone fits into cup like depression of another bone forming a movable joint. Multi-axial movements are possible. This type of joint allows movements along all three axes and in all directions. e.g. Shoulder and hip joint.
3. Hinge joint: In a hinge joint, convex surface of one bone fits into concave surface of another bone. In most hinge joints one bone remains stationary and other moves. The angular opening and closing motion (like hinge) is possible. In this joint only mono-axial movement takes place like flexion and extension. e.g. Elbow and knee joint.
4. Condyloid joint: It is an ellipsoid joint. The convex oval shaped projection of one bone fits into oval shaped depression in another bone. It is a biaxial joint because it permits movement along two axes viz, flexion, extension, abduction, adduction and circumduction is possible. e.g. Metacarpophalangeal joint.
5. Gliding joint: It is a planar joint, where the articulating surfaces of bones are flat or slightly curved. These joints are non-axial because the motion they allow does not occur along an axis or a plane. e.g. Intercarpal and intertarsal joints.
Saddle joint: This joint is a characteristic of Homo sapiens. Here the articular surface of one bone is saddle-shaped and that of other bone fits into saddle (each bone forming this joint have both concave and convex areas). It is a modified condyloid joint in which movement is somewhat more free. It is a biaxial joint that allows flexion, extension, abduction, adduction and circumduction. e.g. Carpometacarpellar joint between carpal (trapezium) and metacarpal of thumb.
[Students are expected to prepare a chart on their own.]
Can you tell? (Textbook Page No. 211)
Question 1.
Human beings can hold an object in a better manner than monkeys. Why?
Answer:
- Humans and monkeys both have five fingers including thumb, however humans can hold an object in better manner than monkeys because humans have highly developed opposable thumbs. The opposable thumb allows better grip.
- The saddle joint in thumb allows free and independent movement to the thumb the carpometacarpellar joint between carpal (trapezium) and metacarpal of thumb makes the thumb opposable. It allows biaxial movements, i.e. flexion – extension and adduction – abduction but not rotation.
[Note: Gorillas, chimpanzees, orangutans and some other variants of apes have opposable thumb.]
Internet my friend. (Textbook Page No. 211)
Question 2.
Now a days we hear from many elderly people that they are undergoing knee replacement surgery. Find out why one has to undergo knee replacement; how it is carried out and how it can be prevented.
Answer:
Knee replacement is done in following cases:
- Osteoarthritis: The cartilage in the knee undergoes degradation. It is caused by many factors such as muscle weakness, aging, obesity, etc.
- Rheumatoid arthritis: It is characterised by inflammation of the synovial membrane, where it starts secreting excess of synovial fluid in the joint. This fluid exerts extensive pressure on the joint and causes severe pain.
- Post-traumatic arthritis: This is caused due to breakage of ligament or cartilage. The breakage can be due to severe injury or accident. It causes severe pain and requires knee replacement.
-
Procedure:
The procedure involves removal of the damaged cartilage or ligament and replaces it with artificial implant made up of either metal, plastic or both. Metal or plastic knee caps are used to cover the knees. The implant is connected to the bone and an artificial knee joint is made between them. - Prevention: Maintaining body weight, exercising regularly, consuming appropriate medications and supplements, etc.
[Students are expected to find out more information about knee replacement on internet]
Find out. (Textbook Page No. 212)
Question 1.
You must have heard of Sachin Tendulkar suffering from ‘tennis elbow’, a cricketer suffering from a disorder named after another game. Can common people too suffer from this disorder? Find out more information about this disorder.
Answer:
- Tennis elbow is caused due to inflammation of tendon which joins muscles of forearm to the bone of upper arm (humerus). It is known as lateral epicondylitis.
- It causes severe pain in the elbow. It occurs due to extensive repetitive movement of hand. This damages the tendon and increases the tenderness of the elbow joint.
- This disorder develops not only in athletes but also in other common people whose job involves extensive movement of hand such as carpenter, painter, plumber, etc.
[Students are expected to find more information about tennis elbow on their own.]